Published - Sat, 22 Oct 2022
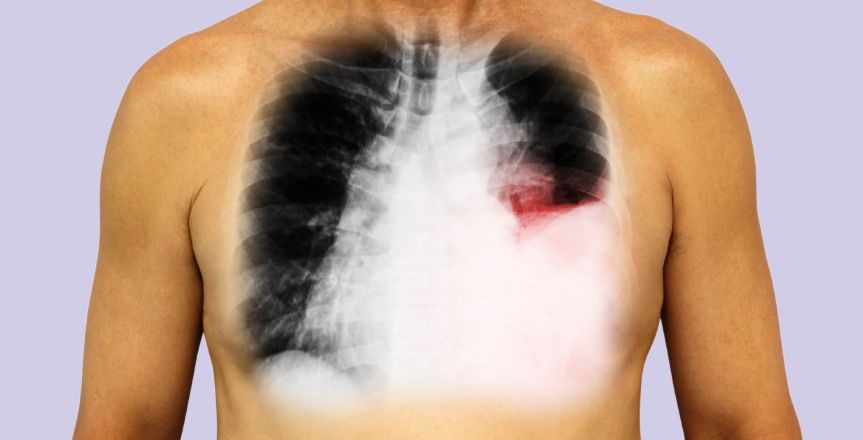
Pleural Effusion
The accumulation of fluid in layers in
the layer between the lungs and chest cavity. A small amount of fluid is
present in this cavity for lubrication during breathing, but too much
accumulation can cause a problem, which is stated as pleural effusion.
Causes
A wide variety of things can cause a
serious membrane effusion which may include
o
Congestive
heart failure.
o
Cirrhosis
o
Pulmonary
embolism
o
Cancer.
o
Kidney
disease
o
Infections:
pneumonia.
o
Autoimmune
conditions. Lupus or rheumatoid arthritis
Symptoms
You may not have any symptoms in case
of a small effusion, but, if there is a large or moderate-sized pleural effusion,
or if there's associated inflammation. Then you may have
o
Shortness
of breath
o
Chest
pain, especially during deep inhalation (This is termed pleuritic pain.)
o
Fever
o
Cough
Types of pleural effusion
"Transudative" and "Exudative" are the 2 main types of pleural effusions
|
Type of Pleural Effusion |
Transdutaive |
Exudative |
|
Cause |
Increased pressure in the blood
vessels can lead to the leaking of fluid into the pleural space
|
The fluid buildup occurs owing to
infection, injury, and the associated inflammation
|
|
Conditions that can give rise to this
effusion type |
>
Congestive
heart failure >
Cirrhosis >
kidney
disease >
Malnutrition
|
>
tuberculosis >
cancer >
inflammatory
conditions, [lupus, or rheumatoid arthritis] >
pneumonia |
Created by

Comments (0)
Search
Popular categories
Latest blogs

All you need to know about Syphilis
Tue, 15 Nov 2022

What is Pemphigus Vulgaris?
Tue, 15 Nov 2022

Know about Scorpion Stings
Sat, 12 Nov 2022
Write a public review